

The initial search resulted in 1,825 papers. After eliminating duplicate studies, 1,240 studies remained. An additional 5 papers were found through other sources. After a detailed screening of titles, abstracts and full texts, we selected 36 studies, including 33 quantitative studies and 3 qualitative studies for the final analysis (Fig. 1).
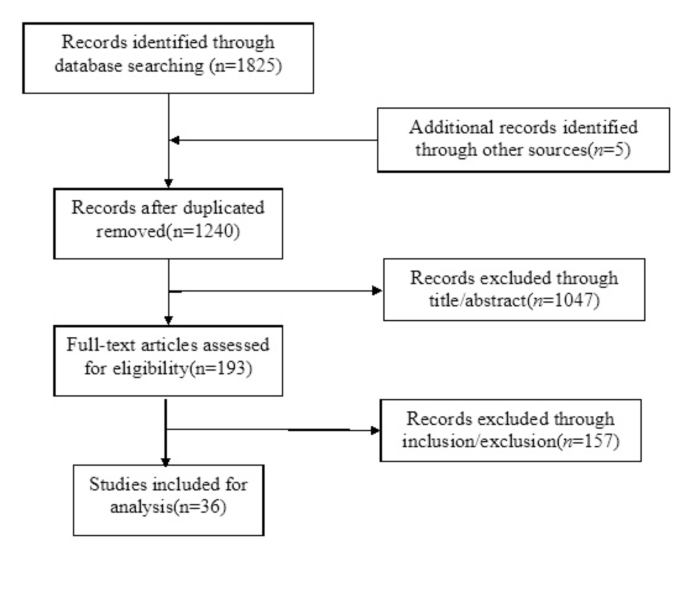
Study selection process of the concept analysis
Use of the concept
Identifying all instances of SWSD in the literature is essential to clarify its scope and deepen understanding of its applications [15]. SWSD is initially defined as a sleep disorder caused by the disruption of normal sleep cycles due to shift work, typically manifests as insomnia and excessive sleepiness [7, 8]. Early research by Regestein revealed that shift work not only disrupts sleep but also triggers broader systemic health problems by interfering with sleep patterns [17], laying the foundation for SWSD to be recognized as a formal sleep disorder. In 2000, the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) expanded the concept to include social and occupational impairments [18], acknowledging SWSD’s significant impact on daily functioning. The International Classification of Sleep Disorders (ICSD) further refined the diagnostic criteria for SWSD. ICSD-2 (2005) provided precise criteria, and ICSD-3 (2014) introduced stricter standards, requiring symptoms to persist for at least three months [19, 20], reflecting SWSD’s multifaceted impact on physical and mental health. As research progressed, SWSD classifications became increasingly detailed. Gumenyuk (2015) proposed categorizing SWSD based on the presence of insomnia and/or excessive sleepiness, while Vanttola (2020) identified three subtypes: insomnia only, both insomnia and excessive sleepiness, and excessive sleepiness only [21, 22]. This classification highlights symptom variability among shift workers, underscoring the need for more personalized diagnostic and treatment approaches. In summary, SWSD has evolved from a focus on sleep disturbances alone to a multidimensional disorder encompassing impacts on health, social interactions, and occupational performance. The ICSD framework remains the primary basis for SWSD diagnosis and research (Table 2).
Defining attributes
The features or phenomena associated with a concept are referred to as the attributes of the concept, which help distinguish it from other phenomena [16]. Attributes of SWSD identified through the analyses included internal/external circadian rhythm imbalance, impaired sleep, multidimensional health problems, and dynamic changes in symptoms.
Internal/external circadian rhythm imbalance
An imbalance between internal and external circadian rhythms represents a core characteristic of SWSD, arising from conflicts between work schedules and the body’s natural sleep-wake cycle. Shift work misaligns the body’s endogenous circadian rhythms with external environmental cues, disrupting the regulation of the suprachiasmatic nucleus (SCN) and the pineal gland. This misalignment ultimately leads to altered melatonin secretion patterns, often manifesting as reduced or shifted melatonin release [24, 25]. Gumenyuk’s research reveals that, in night shift workers, peak melatonin levels are reached during the day rather than at night, causing a substantial misalignment between sleep cycles and work demands, which, in turn, contributes to poor sleep quality [26]. Additionally, studies indicate that night shifts (starting after midnight) and early morning shifts (between 4:00 AM and 7:00 AM) are particularly disruptive to circadian rhythms, thereby exacerbating SWSD symptoms [27].
Impaired sleep
Impaired sleep is also a defining characteristic of SWSD among nurses, typically presenting as insomnia, excessive daytime sleepiness, and reduced sleep quality. Circadian disruptions and irregular melatonin secretion contribute significantly to these symptoms, as night shift nurses often experience heightened difficulty with insomnia and increased daytime sleepiness [28]. Insomnia in this context often includes challenges with sleep onset, sleep maintenance, and early awakening, all of which are commonly reported among shift-working nurses [29]. A study conducted in Spain found that 51.8% of nurses suffer from excessive daytime sleepiness, underscoring the prevalence of this symptom in shift-working populations [30]. Poor sleep quality is another common issue; numerous nurses report insufficient restorative sleep and frequent nighttime awakenings, which can have a deleterious impact on their health and well-being [31, 32].
Multidimensional health issues
Shift work, as a significant environmental stressor, disrupts circadian rhythms and affects hormonal balances closely related to metabolic processes. For example, the secretion of insulin and melatonin declines, while levels of dopamine and norepinephrine increase [33], potentially elevating risks for conditions such as diabetes, cardiovascular diseases, and cancer [1]. Studies indicate that circadian disruptions caused by shift work alter nocturnal melatonin and reproductive hormone levels in women, which has been associated with an increased risk of breast cancer [30]. Wyse’s research further supports that shift workers have a higher prevalence of obesity, diabetes, sleep disorders, and mental health issues [34]. Additionally, a study observed that night-shift nurses tend to consume more snacks, sugary drinks, and alcohol, which correlates with higher incidences of diabetes, cardiovascular symptoms, and gastrointestinal problems [35]. Jaradat also identified elevated psychological stress among shift-working nurses, a factor linked to functional gastrointestinal disorders [36].
Dynamism of symptom changes
The symptoms of SWSD demonstrate dynamic variability, often fluctuating in response to changes in shift schedules. When shift workers discontinue shift work, adverse effects on sleep quality and overall health generally diminish. For instance, a study reported that the prevalence of SWSD among trainee nurses was 35.2% after three months and increased slightly to 37.7% after six months of continuous shifts. After nine months, a two-week period of sufficient rest reduced the prevalence to 14.8% [37]. However, sleep-related symptoms tend to recur once shift schedules are reintroduced, highlighting the recurrent and chronic nature of SWSD in relation to sustained shift work.
Cases of SWSD
Model case
Maria, a nurse with 10 years of intensive care experience, works at least five-night shifts per month. After her shifts, she must care for her three-year-old daughter, and on her days off, she is often obligated to attend to additional commitments, such as teaching and exams. This demanding schedule resulted in a misalignment between her internal circadian rhythm and the external environment, manifesting as a decreased tolerance for night shifts, particularly from 2:00 a.m. to 5:00 a.m. During this time—her peak period of sleepiness—Maria was expected to stay awake. The combination of night shifts and insufficient rest contributed to a significant increase in nighttime insomnia and daytime sleepiness, which in turn limited her social activities and interactions. Over time, these disruptions led to multidimensional health issues, including sleep disorders, endocrine imbalances, and other health complications. Subsequently, Maria enrolled in a three-month mentorship training program organized by her hospital. This program resulted in notable improvements in her sleep quality and social relationships, as she was no longer required to work night shifts, demonstrating a positive shift in her health and well-being (dynamics of symptom change).
Contrary case
A contrary case, which lacks the core attributes of SWSD, is exemplified by James, an anesthesia nurse with 12 years of experience who works at least four-night shifts per month. Prior to his shifts, James takes a restorative nap of one to two hours, which enables him to manage night duties effectively. During shifts, he often takes a brief 30-minute rest between 3:00 a.m. and 5:00 a.m. After completing his night shift, he follows a structured rest schedule by sleeping from 9:00 a.m. to 1:00 p.m. and going to bed before 11:00 p.m., using blackout curtains and disabling his phone and alarm clock to maintain sleep quality. James reports no history of sleep disorders. On his days off following night shifts, he actively participates in social activities and attends to his children’s needs, demonstrating effective adaptation to night shift work and seamless integration of this schedule into his lifestyle.
Antecedents
Antecedents are factors that trigger conceptual events. According to literature analysis, the occurrence of SWSD is based on shift work and arises due to various factors such as the circadian rhythm patterns of shift workers, the nature of the shifts, the number of shifts, and the shift patterns. Therefore, the occurrence of SWSD can be attributed to a variety of factors at both the individual and organizational levels.
Individual factors
Several individual factors contribute to nurses’ sleep quality, including physical and mental health, lifestyle choices, sleep hygiene, and family support [38, 39]. Physical and mental health conditions interact with SWSD in complex ways. Prolonged exposure to shift work can impair physical health and increase negative emotions, which further deteriorate overall well-being and may even prevent shift workers from continuing their roles effectively [40]. During night shifts, lifestyle factors such as excessive eating, drinking, and caffeine intake can overstimulate the sympathetic nervous system, leading to heightened physiological stress [36]. Irregular sleep patterns, engaging in strenuous exercise before bedtime, and sleeping in uncomfortable environments are additional factors that can negatively impact sleep quality [41]. Family support and circadian rhythm type also play a significant role in a nurse’s sleep quality. Circadian rhythms are typically classified into morning and evening types, with morning types showing poorer adaptability to shift work compared to evening types, who are generally better able to adjust to irregular schedules [38]. Furthermore, limited family support and the added responsibility of caring for children make shift workers more susceptible to developing SWSD [24].
Organizational factors
Organizational factors contributing to SWSD include shift type, the interval between shifts (e.g., rapid rotation), shift regularity, the number and duration of night shifts, and the lack of opportunities to nap during night shifts [2]. Rotating or night shifts disrupt the body’s internal clock, making it challenging for individuals to adjust to irregular sleep schedules. Frequent and consecutive night shifts contribute to cumulative sleep deprivation, further impairing sleep quality. Irregular shift schedules, in which nurses frequently alternate between day and night shifts, impede the body’s ability to establish a stable sleep pattern. Collectively, these organizational factors disrupt natural circadian rhythms and the production of sleep-regulating hormones, such as melatonin, exacerbating SWSD symptoms [41].
Consequences
Consequences are events that occur as a result of this concept, they can manifest in aspects such as nurses’ physiological health, psychological well-being, social adaptation, and nursing work.
SWSD on nurses’ physiological health
Shift work, as an environmental stressor, disrupts synchronization between the body’s internal biological clock and external circadian rhythms, leading to sleep-related issues such as insomnia and excessive sleepiness [22]. This misalignment also impacts metabolic hormones, decreasing insulin and melatonin levels while increasing dopamine and norepinephrine, thereby elevating risks for diabetes, cardiovascular disease, and cancer [30]. Molzof’s survey indicates that nurses consume snacks and sugary drinks more frequently during night shifts, which significantly raises the incidence of diabetes, cardiovascular complications, and gastrointestinal disorders [35].
SWSD on nurses’ mental health
Individuals with SWSD commonly experience fatigue, decreased alertness, and cognitive impairment during night shifts. They also often face insomnia and difficulty falling asleep after night shifts, which can lead to adverse emotional states, including anxiety and depression [36, 39]. Research indicates that prolonged exposure to night shifts elevates the likelihood of these negative emotional outcomes, with shift nurses facing a 1.5 times higher risk of depression compared to non-shift nurses [42].
SWSD on nurses’ social adaptability
Irregular work schedules and night shifts often misalign nurses’ social time with that of family and friends, leading to social isolation [1]. Shift work can also conflict with childcare and family responsibilities, creating additional strain. Furthermore, prolonged shift work has been linked to deteriorating mental health, with increased levels of anxiety and depression making social interactions more difficult [43].
SWSD on nursing care
Sleep disorders related to shift work impair nurses’ performance and compromise occupational safety [1]. Working more than 12 h a day or over 40 h per week significantly raises the risk of occupational hazards [44]. Performance notably declines between 4:00 and 8:00 a.m., during which medical errors increase. Nurses working shifts longer than 12 h show reduced vigilance, doubling their risk of medical errors compared to those on shorter shifts [12]. Additionally, SWSD negatively impacts job satisfaction. Studies indicate that as shifts transition from day to permanent night duty, both sleep quality and job satisfaction decline [45]. Shift nurses also experience greater effort-reward imbalances, heightening stress and potentially leading to poorer nursing outcomes.
Empirical referents
Empirical referents are methods used to assess a concept’s definition, attributes, and characteristics [15]. A literature review reveals that no comprehensive instrument currently captures all attributes of SWSD. The Bergen Shift Work Sleep Questionnaire (BSWSQ) is commonly used to evaluate insomnia symptoms among nurses engaged in shift work [46]; however, it cannot definitively attribute these symptoms to shift work alone, necessitating further validation. The Pittsburgh Sleep Quality Index (PSQI), widely utilized internationally to assess sleep quality and disturbances [47], is effective in diagnosing sleep issues yet does not account for sleep patterns across different shifts and may not be suited for specific sleep disorders in shift workers. Other scales, including the Epworth Sleepiness Scale, Stanford Sleepiness Scale, and Karolinska Sleepiness Scale, measure sleepiness levels but have limited capacity for detecting underlying sleep disorders [48]. Additionally, tools like the Athens Insomnia Scale and the Insomnia Severity Index are useful for identifying insomnia and assessing intervention efficacy but lack sufficient specificity for SWSD [49]. Thus, further research should focus on developing instruments that comprehensively measure SWSD’s characteristics and severity in the nursing context. A universally validated tool would improve nurses’ awareness of SWSD and foster broader discussions on this issue within the nursing profession.
Definition of the concept
Combining the analysis of the prerequisite conditions, attribute characteristics, influencing factors, adverse consequences, and related case introductions and analyses for SWSD, the concept of sleep disorders in nurses working shifts can be defined as a phenomenon that adversely affects the sleep and health of shift nurses, which is influenced by shift patterns, frequency, and duration, as well as lifestyle, family support, and sleep hygiene. Shift work is a prerequisite for SWSD, sleep disturbance is a core conceptual attribute, and impaired physical and mental health is an endpoint. A conceptual model is shown in Fig. 2.

The antecedents, attributes and consequences of SWSD
link