



The study included 200 participants, 140 females (70.0%) and 60 males (30.0%). Most participants age 20–30 years (n = 116, 58.0%), followed by those aged 30–40 years (n = 57, 28.5%). The majority were pediatric residents (n = 84, 42.0%) and pediatric nurses (n = 72, 36.0%). The mean professional experience was 6.4 years (SD = 6.1), ranging from less than 1 to 30 years. Most participants had never been hospitalized (n = 124, 62.0%), and 139 (69.5%) were not parents. Among those with children, 27 (31.4%) reported that their child had been hospitalized. With respect to sleep education, 121 (60.5%) participants received 0–5 h. 102 (51.0%) deemed this inadequate. Ninety-three (46.5%) addressed sleep-related issues 1–3 times/month (Table 1).
Major key knowledge items related to sleep-disturbing factors are summarized (Table 2).
The attitudes and perceptions of the participants toward child and parent sleep were discussed. For children, the importance of adequate sleep for a child’s health had a mean score of 3.74 (SD = 0.604), with a median score of 4, indicating substantial agreement. The participants believed that children sleep less in the hospital than at home, with a mean of 3.38 (SD = 0.753) and a median of 4. There was moderate agreement regarding how many hours pediatric patients need to sleep (mean = 3.03, SD = 0.795, median = 3). The participants agreed that maximizing pediatric sleep aids recovery (mean = 3.43, SD = 0.712, median = 4) but felt less confident in knowing how to help children sleep better in the hospital (mean = 2.69, SD = 0.823, median = 3). They were somewhat neutral in their efforts to help children sleep (mean = 3.11, SD = 0.792, median = 3). With respect to parental sleep, participants moderately agreed that adequate sleep for parents is essential for their child’s health (mean = 3.36, SD = 0.722, median = 3) and that parents sleep less in the hospital (mean = 3.43, SD = 0.740, median = 4). There was less certainty about the importance of maximizing parent sleep for child recovery (mean = 3.16, SD = 0.790, median = 3). Confidence in helping parents sleep better in the hospital was low (mean = 2.57, SD = 0.818, median = 3), and participants felt only moderately engaged in assisting parents to sleep (mean = 2.89, SD = 0.807, median = 3). (Tables 3 and 4).
Participants’ knowledge of the effectiveness of various interventions to reduce noise at night in the hospital was assessed. Staff education was rated as “Very Effective” by 83 participants (41.5%) and “Effective” by 103 (51.5%), with only 14 (7.0%) being unsure or considering it ineffective. Posting signs about noise reduction were considered “very effective” by 67 participants (33.5%) and “Effective” by 94 (47.0%), whereas 39 (19.5%) were unsure or found it ineffective. Turning pagers to vibrate was rated “Very Effective” by 56 participants (28.0%) and “Effective” by 81 (40.5%), but 63 (31.5%) were unsure. Turning down phone ringers was seen as “Very Effective” by 64 (32.0%) and “Effective” by 101 (50.5%), with 35 (17.5%) unsure. Lowering staff voices was rated “Very Effective” by 79 (39.5%) and “Effective” by 99 (49.5%), with 22 (11.0%) being unsure. Closing patient doors was viewed as the most effective intervention, with 122 (61.0%) rating it as “Very Effective” and 69 (34.5%) as “Effective”. Reducing unnecessary monitors and alarms was also considered highly effective, with 110 (55.0%) rating it as “Very Effective” and 70 (35.0%) as “Effective.” (Table 5).
To measure different possible related factors, we aimed to assess the associations between knowledge of pediatric healthcare workers’ interventions to reduce noise at night and various demographic and professional characteristics. Gender did not significantly affect knowledge level (p = 0.711), with similar proportions of females (52.1% with low knowledge) and males (55.0% with low knowledge). Age also showed no significant association (p = 0.903), with the majority of each age group having low knowledge. Similarly, pediatric caregiver role (p = 0.918), years of experience (p = 0.452), hospitalization history (p = 0.616), and being a parent (p = 0.101) were not significantly associated with knowledge level. However, the number of hours of sleep was significantly associated with knowledge levels (p = 0.022). A greater percentage of participants with 0–5 h of sleep had high knowledge (51.2%). There was no significant difference in knowledge levels based on perceived adequacy of sleep (p = 0.545) or the frequency of addressing sleep-related issues in clinical practice (p = 0.323). In logistic regression analysis, sleep-education hours were the only variable significantly associated with higher knowledge (p = 0.022). Other demographic and professional characteristics were not significant predictors. (Table 6)
We explored the associations between attitudes and perceptions scores and various participant features. Gender was not significantly associated with the attitude and perception scores (p = 0.498), with females scoring a mean of 34.61 (SD = 5.21) and males scoring slightly higher at 35.13 (SD = 4.54). There were no significant differences in the scores across the age groups (p = 0.484), with the highest mean score of 23.28 (SD = 2.98) in the 50–70 years age group. Among pediatric caregivers, pediatric consultants/fellows had the highest mean score of 36.27 (SD = 5.25), but this difference was not significant (p = 0.187). Compared with those with fewer years, those with more than 5 years of experience scored slightly higher (mean = 35.38, SD = 5.08), but this difference was not statistically significant (p = 0.100). Hospital history and being a parent had no significant effect on scores (p = 0.888 and p = 0.109, respectively), although parents tended to score slightly higher. Sleep hours were not significantly associated with scores (p = 0.950). Participants who perceived their sleep education as adequate had a higher mean attitude/perception score; however, this difference did not reach statistical significance (p = 0.080). Finally, those addressing sleep-related issues more frequently (> 1/week) had a higher mean score (36.07, SD = 5.86), although this association was not significant (p = 0.157). (Table 7)
Various disruptive factors for sleep in the hospital were assessed as addressed by healthcare workers included in the study. The most critical disruptive factors for sleep are blood draws or other tests (mean = 3.36), closely followed by pain (mean = 3.31) and equipment alarms (mean = 3.1). Noise from all sources also scored highly, with a mean of 3.06. Other disruptions included vital sign checks (mean = 2.98) and feeling anxious (mean = 2.93). The lower-rated disruptions included respiratory therapist interruption (mean = 2.66), staff conversation (mean = 2.58), and continuous pulse oximetry (mean = 2.44). (Fig. 1)

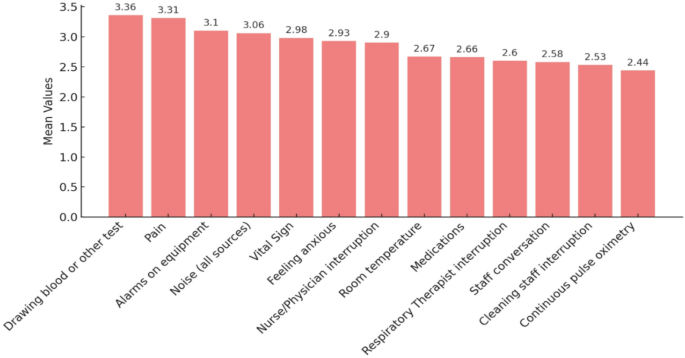
Disruptive factors for sleep in hospitals as perceived by the healthcare workers (n = 200).
Interventions to address sleep issues were explored in clinical practice among participants who faced many cases (n = 136). The most common intervention was providing advice related to sleep hygiene and sleep practices (77.2%). Sleep medications such as melatonin are used by 62.5%, whereas behavioral interventions are applied by 61.0%. Light therapy was another notable intervention used by 42.6% of the participants. Referral to a sleep clinic is less common, with only 18.4% making such referrals and 4.4% reporting using other interventions. (Fig. 2)

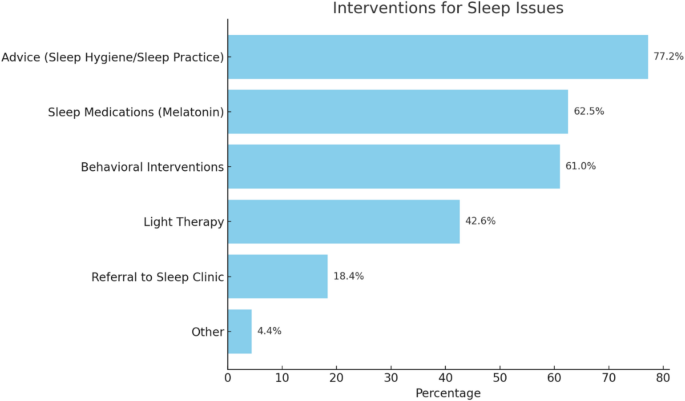
Different interventions to address sleep issues in your clinical practice if you face many cases (n = 136, sometimes too often).
link